It is the Global Take Over and it is hear!! Don’t worry about which country is refenced in any of the articles or videos below. It does not matter because, as I said, IT IS GLOBAL. The very same things are coming to every country in the WORLD and they are coming fast!!
It is not like they didn’t know, or that we weren’t warned. For the most part, people preferred not to think about it, like it would somehow go away, if we just ignored it. Well, now there is no way to stop it and there will be nowhere to hide.
Truthers have been warning us that the World Elite are plotting to kill us all, though it sounds so absurd it is the TRUTH.
Killing the “poor” has been a reoccurring theme in books, songs and movies, for decades.
Those who do not know God Love Death!
36 But he that sinneth against me wrongeth his own soul: all they that hate me love death.

“The sun beams down on a brand new day,
No more welfare tax to pay,
Unsightly slums gone up in flashing light.
Jobless millions whisked away,
At last we have more room to play,
All systems go to kill the poor tonight.”
When someone takes Lyndon Johnson‘s “War on Poverty” a bit too literally and fights poverty with the most dubious and immoral methods imaginable.
Instead of seeking to eliminate poverty by educating and supporting the impoverished so they can attain a greater quality of life and income, some believe it would be easier to eliminate poor people with mass executions.
On the plus side, this approach would have a whopping 100% success rate. On the other hand, it’s horrifically unethical, and also counter-productive to a more prosperous economy (if you kill workers of low-paying jobs, now nobody is doing their job, which hurts the economy; also, many businesses would be doomed without poor customers.)
Less lethal alternatives may involve poverty being made illegal and poor people being treated as criminals, possibly forced into slave labor or a similar venture so that they can be “put to better use.” This has some historical precedence with things like the workhouse system in 1800s Britain, but fiction will usually take it to even more horrifying extents.
In either case, this trope is usually rife with sociopolitical and socioeconomic Satire and Symbolism, exaggerating how Upper Class Twits and other wealthy elites both want to view the lower classes and, more cynically, how they may actually view such groups. In this fashion, the concept could be used as a form of Black Comedy. To other extents, this could involve a character crossing the Moral Event Horizon and establishing themself as a Politically Incorrect Villain. It might also lead to A Nazi by Any Other Name or a High-Class Cannibal.
A Sub-Trope of The Social Darwinist and Slobs Versus Snobs.
Compare Disposable Vagrant, for the murder/exploitation of impoverished people on a smaller/more discreet scale For Science! or other personal motivations.
Contrast Eat the Rich.
spacer
TROPE Definition & Meaning – Dictionary.com
spacer
Most-read 2022: Why is Canada euthanising the poor?

We’re finishing the year by republishing our ten most popular articles from 2022. Here’s number one: Yuan Yi Zhu’s piece from April on Canada’s euthanasia policy.
There is an endlessly repeated witticism by the poet Anatole France that ‘the law, in its majestic equality, forbids the rich as well as the poor to sleep under bridges, to beg in the streets, and to steal bread.’ What France certainly did not foresee is that an entire country – and an ostentatiously progressive one at that – has decided to take his sarcasm at face value and to its natural conclusion.
Since last year, Canadian law, in all its majesty, has allowed both the rich as well as the poor to kill themselves if they are too poor to continue living with dignity. In fact, the ever-generous Canadian state will even pay for their deaths. What it will not do is spend money to allow them to live instead of killing themselves.
As with most slippery slopes, it all began with a strongly worded denial that it exists. In 2015, the Supreme Court of Canada reversed 22 years of its own jurisprudence by striking down the country’s ban on assisted suicide as unconstitutional, blithely dismissing fears that the ruling would ‘initiate a descent down a slippery slope into homicide’ against the vulnerable as founded on ‘anecdotal examples’. The next year, Parliament duly enacted legislation allowing euthanasia, but only for those who suffer from a terminal illness whose natural death was ‘reasonably foreseeable’.
Despite the government‘s insistence that assisted suicide is about individual autonomy, it has also kept an eye on the fiscal advantages
It only took five years for the proverbial slope to come into view, when the Canadian parliament enacted Bill C-7, a sweeping euthanasia law which repealed the ‘reasonably foreseeable’ requirement – and the requirement that the condition should be ‘terminal’. Now, as long as someone is suffering from an illness or disability which ‘cannot be relieved under conditions that you consider acceptable’, they can take advantage of what is now known euphemistically as ‘medical assistance in dying’ (MAID for short) for free.
Soon enough, Canadians from across the country discovered that although they would otherwise prefer to live, they were too poor to improve their conditions to a degree which was acceptable.
Not coincidentally, Canada has some of the lowest social care spending of any industrialised country, palliative care is only accessible to a minority, and waiting times in the public healthcare sector can be unbearable, to the point where the same Supreme Court which legalised euthanasia declared those waiting times to be a violation of the right to life back in 2005.
Many in the healthcare sector came to the same conclusion. Even before Bill C-7 was enacted, reports of abuse were rife. A man with a neurodegenerative disease testified to Parliament that nurses and a medical ethicist at a hospital tried to coerce him into killing himself by threatening to bankrupt him with extra costs or by kicking him out of the hospital, and by withholding water from him for 20 days. Virtually every disability rights group in the country opposed the new law. To no effect: for once, the government found it convenient to ignore these otherwise impeccably progressive groups.
Since then, things have only gotten worse. A woman in Ontario was forced into euthanasia because her housing benefits did not allow her to get better housing which didn’t aggravate her crippling allergies. Another disabled woman applied to die because she ‘simply cannot afford to keep on living’. Another sought euthanasia because Covid-related debt left her unable to pay for the treatment which kept her chronic pain bearable – under the present government, disabled Canadians got $600 in additional financial assistance during Covid; university students got $5,000.
When the family of a 35-year-old disabled man who resorted to euthanasia arrived at the care home where he lived, they encountered ‘urine on the floor… spots where there was feces on the floor… spots where your feet were just sticking. Like, if you stood at his bedside and when you went to walk away, your foot was literally stuck.’ According to the Canadian government, the assisted suicide law is about ‘prioritis[ing] the individual autonomy of Canadians’; one may wonder how much autonomy a disabled man lying in his own filth had in weighing death over life.
Despite the Canadian government’s insistence that assisted suicide is all about individual autonomy, it has also kept an eye on its fiscal advantages. Even before Bill C-7 entered into force, the country’s Parliamentary Budget Officer published a report about the cost savings it would create: whereas the old MAID regime saved $86.9 million per year – a ‘net cost reduction’, in the sterile words of the report – Bill C-7 would create additional net savings of $62 million per year. Healthcare, particular for those suffering from chronic conditions, is expensive; but assisted suicide only costs the taxpayer $2,327 per ‘case’. And, of course, those who have to rely wholly on government-provided Medicare pose a far greater burden on the exchequer than those who have savings or private insurance.
spacer
Now we all know that the world is facing an aging society. The cost of providing care for our senior citizens is rising and though we had years to prepare for this inevitability… very little has been done to offset it.
spacer


It is not just the seniors of our society that are finding themselves in poverty, also among the poorest are children. Helpless children. Sadly, our Godless, self-centered society has no compassion on the most vulnerable among us.
spacer
Child poverty report
spacer
![]()
More than one third of children in Toronto Centre are living in a low-income household. Mark McAllister speaks to the authors of a …
A single mother of three has good credit and is employed full-time, but was briefly homeless due to Toronto’s rental market.
![]()
289K subscribers

![]()
spacer
spacer
spacer
spacer
spacer
spacer

![]() Context: Beyond the Headlines
Context: Beyond the Headlines
Canada has a poverty problem. The numbers are staggering. 3.2 million Canadians live in poverty. And one in five children are …


![]()
137K subscribers
 / ssadisabili. .
/ ssadisabili. .


![]()
131K subscribers49K views Streamed 15 hours ago #ushousingmarket #useconomy #realestatenews
spacer
ALL our “BRILLIANT” leaders, all the THINK TANKS, all our Corporate Heads, technical and financial geniuses, all our Non-Government Organizations and Social Committees, all our elected Officials and World Delegates, all the SuperComputers using AI technology and their simulations to model the future, and all the Nobility and all the billionaires who stuff their bank accounts with the money they made of the labor of the those they consider below them have a solution to all the world’s problems… KILL the Poor, the Sick, the Disabled, and ALL THOSE THEY SEE AS WORTHLESS EATERS!!
Check out the following related Post:
We kill babies, Now we will kill the Mentally Handicapped… who is next?
spacer
Half of all Canadians say there are too many immigrants: poll
Concerns over immigration are primarily about the economy rather than fears about immigrants changing the social fabric of Canada, the poll suggests

National Poverty in America Awareness Month: January 2024
Key Stats
Source: U.S. Census Bureau, Current Population Survey, Annual Social and Economic Supplement
Figures, Official Poverty Measure:
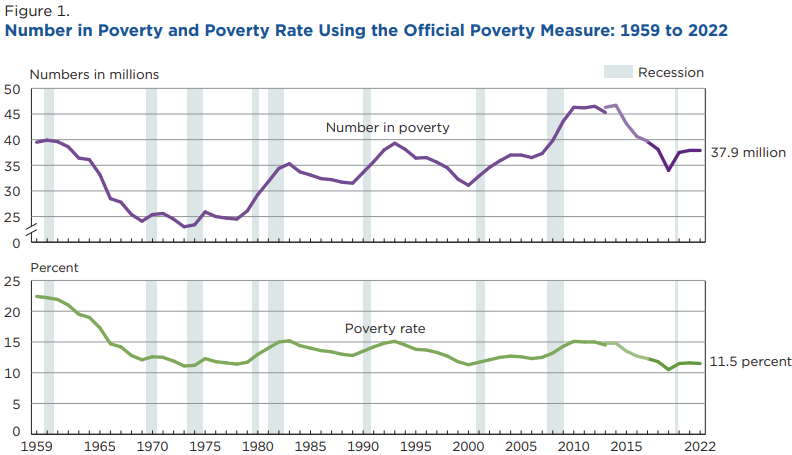
Note: Figure 1 shown above is cropped. Click on the image for the full figure, including notes and source.
spacer
It is not like they did not see this come, or that they did not have time to prepare…but even beyond that…they have been largely responsible for the circumstances.
Poverty in the United States
Poverty is the human condition of being unable to obtain or provide a standard level of food, water and/or shelter for you or your family.
It exists in every country to varying degrees and is unlikely to disappear any time soon. The United States is considered the richest country in the world, and yet 37.9 million (11.5%) of its residents live in poverty. That is the understatement of the year folks!!
Poverty is measured in two ways – absolute poverty and relative poverty.
Absolute poverty looks at the goods and services someone (or a family) cannot obtain.
Relative poverty looks at the context of the need, how one social group compares to others.
The official method of calculating America’s poverty levels was developed in the 1960s and has not been refined substantially since then. Critics maintain that the government overstates the U.S. poverty level because it counts people as impoverished who in generations past, would be considered as not living in poverty.
The highest poverty rate on record was 22% (1950s). The lowest was 10.5% (2019).
Absolute Poverty
Absolute poverty is a measure of the minimal requirements necessary to afford the minimal standards of life-sustaining essentials — food, clothing, shelter, clean water, sanitation, education and access to health care.
The standards are consistent over time and are the same in different countries. For example, one absolute measurement is the percentage of a population that consumes enough food daily to sustain the human body. This standard – 2,000 – 2,500 calories per day – is applied worldwide and across all cultures.
The World Bank defines poverty in absolute terms:
- People anywhere in the world who are living on less than $1.90 per day are living in extreme poverty.
- People living on less than $3.20 per day in lower middle-income countries and less than $5.50 in upper middle-income countries are living in moderate poverty.
For instance, in 2017, 6.5 million people in Europe and Central Asia lived in extreme poverty, compared with almost 431 million in Sub-Saharan Africa.
Relative Poverty
Relative poverty is a measurement of income inequality within a social context. It does not measure hardship or material deprivation, but rather the disparities of wealth among income groups.
For example, in the United States, a household that has a refrigerator, televisions, and air conditioning can be considered impoverished if its income falls below a certain threshold. In other countries, those households might be thought of as wealthy.
Poverty Lines and Measures of Income Inadequacy in the United States Since 1870: Collecting and Using a Little-Known Body of Historical Material, by Gordon M. Fisher
A paper presented October 17, 1997,
at the 22nd Meeting of the Social Science History Association
Washington, D.C.
spacer
If you doubt that our world leaders have been caught unprepared for our current predicament, read on my friend. They have been spent decades even centuries collecting, classifying, measuring and predicting. Then KNOW exactly what is happening and why. I would venture to say that they have manipulated the circumstances to bring us to this point.
spacer
 |
HISTORY |
NIA (National Institute of Aging) was formally established in 1974 but has much earlier origins. This timeline features information about major milestones in NIA’s history. For a more comprehensive history, view NIA in the NIH Almanac.
Browse our history by timeframes:
2020s | 2010s | 2000s | 1990s | 1980s | 1970s | Earlier Origins
Learn about NIA’s funded and conducted high-impact scientific advances in aging and dementia research.

2020s
- 2021: NIA relaunches Alzheimers.gov to connect people with information and resources from across the federal government.
- 2020: NIA and the National Institute of Neurological Disorders and Stroke (NINDS) announce the Roy Blunt Center for Alzheimer’s and Related Dementias (CARD). CARD officially opened its doors in 2022.
2010s
- 2018: NIA releases the Together We Make the Difference: National Strategy for Recruitment and Participation in Alzheimer’s and Related Dementias Clinical Research.
- 2017: NIA launches the Alzheimer’s & Dementia Outreach, Recruitment & Engagement (ADORE) Resources to support research recruitment efforts.
- 2017: NIA holds the first National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers.
- 2017: NIH launches the Alzheimer’s Disease Research Implementation Milestone Database to show research implementation plans and progress toward meeting the goals of the National Plan to Address Alzheimer’s Disease.
- 2016: The Alzheimer’s Disease Preclinical Efficacy Database (AlzPED) is established.
- 2015: NIA presents the first-ever NIH Professional Judgment Budget for Alzheimer’s disease and related dementias. Submitted to the President and then Congress annually, the budget estimates additional future funding needed to most effectively leverage promising scientific opportunities in dementia research.
- 2014: NIH joins public and private partners to launch what is now known as the Accelerating Medicines Partnership Program® for Alzheimer’s Disease (AMP®-AD) to transform the development of new diagnostics and treatments for Alzheimer’s disease.
- 2013: NIA hosts the first NIH Summit on Advances in Geroscience: Impact on Healthspan and Chronic Disease.
- 2013: The President’s Alzheimer’s Disease Research Initiative is created.
- 2013: NIA joins NINDS to host the first Alzheimer’s Disease-Related Dementias Research (ADRD) Summit.
- 2012: NIA launches the International Alzheimer’s and Related Dementias Research Portfolio (IADRP) to capture the full spectrum of federal and non-federal research investments.
- 2012: HHS issues the National Plan to Address Alzheimer’s Disease, as outlined by the National Alzheimer’s Project Act (NAPA).
- 2012: NIA hosts the first Alzheimer’s Disease Research Summit.
- 2011: The Trans-NIH Geroscience Interest Group is formed to enhance opportunities to explore the intersection between aging biology and the biology of diseases that are of interest to the various NIH Institutes and Centers.
- 2011: NAPA is signed into law and NIA joins the federal Advisory Council on Alzheimer’s Research, Care, and Services as an ex officio member.
2000s
- 2008: NIA launches the Dominantly Inherited Alzheimer Network, an international research effort focused on a rare form of inherited Alzheimer’s.
- 2005: NIA established the Alzheimer’s Disease Preclinical Drug Development program.
- 2004: NIA launches the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study.
- 2004: NIA joins public and private partners to fund the Alzheimer’s Disease Neuroimaging Initiative.
- 2003: NIA and the American Federation for Aging Research establishes the Paul B. Beeson Career Development Awards in Aging Research program.
- 2003: NIA and the National Library of Medicine (NLM) unveils NIHSeniorhealth.gov, a health and wellness website designed to increase accessibility of resources for older adults and caregivers. In 2017, the content was moved to the NIA website.
- 2002: The Interventions Testing Program (ITP) launches at NIA to identify agents that extend lifespan and healthspan in mice.
- 2002: NIA partners with the Italian National Research Council and develops the SardiNIA Project.

1990s
- 1997: NIA establishes the Resource Centers for Minority Aging Research.
- 1995: NIA establishes the Nathan Shock Centers of Excellence.
- 1994: NIA establishes the Centers on the Demography and Economics of Aging.
- 1994: The Study of Women’s Health Across the Nation (SWAN) begins as a collaboration between NIA, the National Institute of Nursing Research, the NIH Office of Research on Women’s Health, and the National Center for Complementary and Alternative Medicine.
- 1993: NIA launches the Longevity Assurance Genes Initiative, which will lead to the creation of the Longevity Consortium in 2004.
- 1993: Dr. Richard J. Hodes is named NIA director.
- 1993: NIA funds six Exploratory Centers for Minority Aging and Health Promotion, collaborating with the NIH Office of Research on Minority Health, which later becomes the Resource Centers for Minority Aging Research in 1997.
- 1993: Congress authorizes the establishment of the Edward R. Roybal Centers for Translation Research in the Behavioral and Social Sciences of Aging.
- 1992: NIA establishes the Health and Retirement Study.
- 1991: NIA establishes the Alzheimer’s Disease Cooperative Study.
1980s
- 1988: Congress passes PL 100-607 establishing the Geriatric Research and Training Centers (GRTC) on November 4, 1988, which is later renamed to the Claude D. Pepper Older American Independence Centers.
- 1987: NIA holds its first Summer Institute, which will later be renamed the Butler-Williams Scholars Program.
- 1987: NIA holds the first annual Florence S. Mahoney Lecture on Aging.
- 1986: Congress passes PL 99-660, section 951-952, authorizing the establishment of NIA’s Alzheimer’s Disease Education and Referral (ADEAR) Center on Nov. 14, 1986, now named the Alzheimer’s and related Dementias Education and Referral Center.
- 1984: NIA establishes the first Alzheimer’s Disease Centers. There are now more than 30 Alzheimer’s Disease Research Centers across the United States.
- 1983: Dr. T. Franklin Williams takes the helm as NIA’s director.
1970s
- 1976: Dr. Robert N. Butler is appointed as the first NIA director.
- 1975:The Baltimore Longitudinal Study of Aging, which launched in 1958, moves from NIH’s National Heart Institute to NIA.
- 1975: NIA holds the first meeting of the National Advisory Council on Aging (NACA).
- 1974: Congress passes Public Law (PL) 93-296 authorizing the establishment of a National Institute on Aging on May 31, 1974, and NIA is officially established on Oct. 7, 1974.

Earlier Origins
- 1971: The White House Conference on Aging once again recommends the creation of a separate National Institute on Aging.
- 1968: The Division of General Medical Sciences has responsibility for research grant projects in aging. Aging-related research is conducted and supported throughout NIH.
- 1968: Construction of the Gerontology Research Center in Baltimore is completed.
- 1967: The Gerontology Research Center in Baltimore, long a part of the National Heart Institute, is transferred to NICHD.
- 1965: The Older Americans Act establishes the Administration on Aging as “the Federal focal point for activities in aging.”
- 1963: The National Institute of Child Health and Human Development is established to focus on health issues across the life course, including in old age. President John F. Kennedy remarks, “For the first time, we will have an Institute to promote studies directed at the entire life process rather than toward specific diseases or illnesses.”
- 1962: The Gerontology Research Center Nathan Shock Laboratory facility is donated to NIH by the City of Baltimore (deed dated 12/6/62; recorded 2/1/63).
- 1961: The first White House Conference on Aging recommends the creation of an Aging Institute. Its report reads, in part, “a National Institute of Gerontology should be set up within the National Institutes of Health to conduct research on aging; Federal financial support should be increased for biomedical research in governmental agencies, universities, hospitals, research centers and for building necessary facilities; human population laboratories should be established to study problems associated with aging.”
- 1959: A Section on Aging, headed by James E. Birren, is established within NIMH.
- 1959: Aging research conducted through NIH intramural programs (Gerontology Branch of the National Heart Institute and NIMH Section on Aging).
- 1959: Almost 600 research and training grants on aging are underway through the Center for Aging Research, “the focal point for information on the NIH activities in gerontology.”
- 1958: Baltimore Longitudinal Study of Aging is established.
- 1956: Federal Council on Aging is convened.
- 1956: TheDepartment of Health, Education, and Welfare has a Special Staff on Aging; the Center for Aging Research, which exists within the National Institute of Mental Health (NIMH).
- 1951: In his Trends in Gerontology, Dr. Shock outlines his recommendations for an Institute of Gerontology.
- 1950: President Harry S. Truman convenes the First National Conference on Aging.
- 1948: The Gerontology Branch is moved to the National Heart Institute.
- 1941: The Unit on Aging (eventually, later the Gerontology Branch) moves to Baltimore City Hospital under the direction of Nathan Shock.
- 1941: Surgeon General Thomas Parran forms the National Advisory Committee on Gerontology.
- 1940: A Unit on Aging, headed by Edward J. Stieglitz, is established in the NIH Division of Chemotherapy.
- 1930: Congress changes the name of the Hygienic Laboratory to the National Institute of Health.
- 1887: A federal research laboratory, known as the Laboratory of Hygiene, is established at the Marine Hospital, Staten Island, N.Y., in August, for research on cholera and other infectious diseases. It will be renamed the Hygienic Laboratory in 1891.
Sources:
spacer
Chapter 13. Aging and the Elderly
Nov 6, 2014
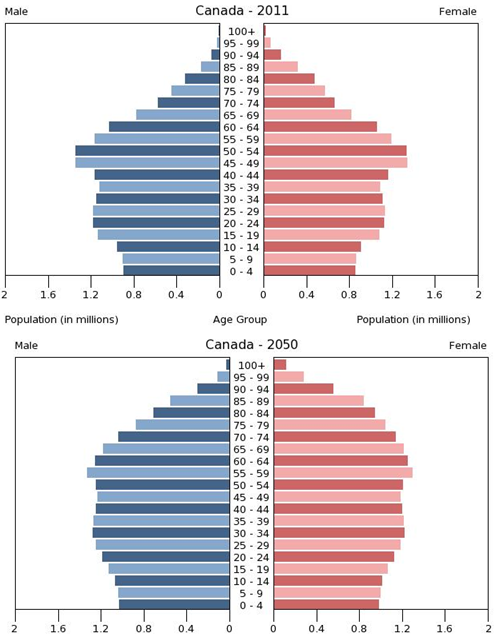
The first census in Canada was conducted in 1666 on the colony’s 3,215 inhabitants and included questions about age as well as sex, marital status, and occupation. Since the first national census in 1871, the Canadian government has been tracking age in the population every 10 years (Statistics Canada 2013a). Age is an important factor to analyze with accompanying demographic figures, such as income and health. The population pyramid below shows projected age distribution patterns for the next several decades.
Statisticians use data to calculate the median age of a population, that is, the number that marks the halfway point in a group’s age range. In Canada, the median age is about 40 (Statistics Canada 2013b). That means that about half of Canadians are under 40 and about half are over 40. The median age of women is higher than men, 41.1 compared to 39.4, due to the persistent higher life expectancy of women (although the gap between genders has been diminishing).
Overall the median age of Canadians has been increasing, indicating that the population as a whole is growing older. It is interesting to note, however, that the proportion of senior citizens in Canada is lower than most of the other G8 countries. In 2013, 15.3 percent of Canadians were over 65 while 25 percent of Japanese, 21 percent of Germans, 21 percent of Italians, 17 percent of French, and 16 percent of British were over 65. Only the United States (14 percent) and Russia (13 percent) had lower proportions (Statistics Canada 2013c).
A cohort is a group of people who share a statistical or demographic trait. People belonging to the same age cohort were born in the same time frame. The population pyramids in Figure 13.3 show the different composition of age cohorts in the population, comparing the population in 2011 with figures projected for 2050. The bulge in the pyramid clearly becomes more rounded in the future, indicating that the proportion of senior cohorts will continue to increase with respect to the younger cohorts in the population. Understanding a population’s age composition can point to certain social and cultural factors and help governments and societies plan for future social and economic challenges. This is key to planning for everything from the funding of pension plans and health care systems to calculating the number of immigrants needed to replenish the workforce.
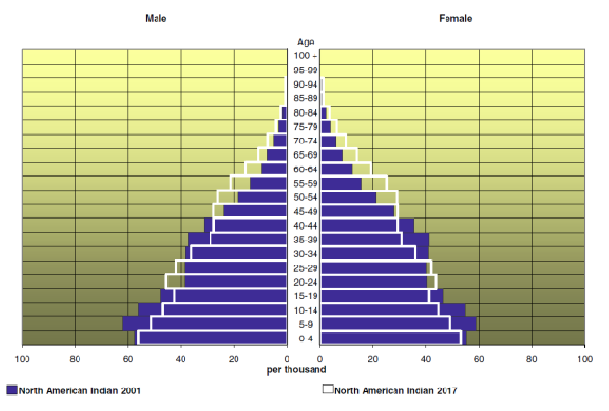
The population pyramid in Figure 13.4 compares the age distribution of the aboriginal population of Canada in 2001 to projected figures for 2017. It is much more pyramidal in form than the graphs for the Canadian population as a whole (see Figure 13.3) reflecting both the higher birth rate of the aboriginal population and the lower life expectancy of aboriginal people. The aboriginal population is much younger than the Canadian population as a whole, with a median age of 24.7 years in 2001 (projected to increase to 27.8 in 2017). Sociological studies on aging might help explain the difference between Native American age cohorts and the general population. While Native American societies have a strong tradition of revering their elders, they also have a lower life expectancy because of lack of access to quality health care.
Phases of Aging: The Young-Old, Middle-Old, and Old-Old
In Canada, all people over age 18 are considered adults, but there is a large difference between a person aged 21 and a person who is 45. More specific breakdowns, such as “young adult” and “middle-aged adult,” are helpful. In the same way, groupings are helpful in understanding the elderly. The elderly are often lumped together, grouping everyone over the age of 65. But a 65-year-old’s experience of life is much different than a 90-year-old’s.
The older adult population can be divided into three life-stage subgroups: the young-old (approximately 65–74), the middle-old (ages 75–84), and the old-old (over age 85). Today’s young-old age group is generally happier, healthier, and financially better off than the young-old of previous generations. In North America, people are better able to prepare for aging because resources are more widely available. (Now that is certainly not true today, it may or may not have been in 2014, but today, totally false.)
Also, many people are making proactive quality-of-life decisions about their old age while they are still young. In the past, family members made care decisions when an elderly person reached a health crisis, often leaving the elderly person with little choice about what would happen. The elderly are now able to choose housing, for example, that allows them some independence while still providing care when it is needed. Living wills, retirement planning, and medical powers of attorney are other concerns that are increasingly handled in advance.
However, the gender imbalance in the sex ratio of men to women is increasingly skewed toward women as people age. In 2013, 67 percent of Canadians over the age of 85 were women (Statistics Canada 2013b). This imbalance in life expectancy has larger implications because of the economic inequality between men and women. The population of old-old women are the cohort with the greatest needs for care, but because many women did not work outside the household during their working years and those who did earned less on average than men, they receive the least retirement benefits.
The Greying of Canada

What does it mean to be elderly? Some define it as an issue of physical health, while others simply define it by chronological age. The Canadian government, for example, typically classifies people aged 65 years old as elderly, at which point citizens are eligible for federal benefits such as Canada Pension Plan and Old Age Security payments. The World Health Organization has no standard, other than noting that 65 years old is the commonly accepted definition in most core nations, but it suggests a cut-off somewhere between 50 and 55 years old for semi-peripheral nations, such as those in Africa (World Health Organization 2012). CARP (formerly the Canadian Association of Retired Persons, now just known as CARP) no longer has an eligible age of membership because they suggest that people of all ages can begin to plan for their retirement. It is interesting to note CARP’s name change; by taking the word “retired”out of its name, the organization can broaden its base to any older Canadians, not just retirees. This is especially important now that many people are working to age 70 and beyond.
There is an element of social construction, both local and global, in the way individuals and nations define who is elderly; that is, the shared meaning of the concept of elderly is created through interactions among people in society. This is exemplified by the truism that you are only as old as you feel.
Demographically, the Canadian population over age 65 increased from 5 percent in 1901 (Novak 1997) to 14.4 percent in 2011. Statistics Canada estimates that by 2051 the percentage will increase to 25.5 percent (Statistics Canada 2010). This increase has been called “the greying of Canada,” a term that describes the phenomenon of a larger and larger proportion of the population getting older and older.
There are several reasons why Canada is greying so rapidly. One of these is life expectancy: the average number of years a person born today may expect to live. When reviewing Statistics Canada figures that group the elderly by age, it is clear that in Canada, at least, we are living longer. Between 1983 and 2013, the number of elderly citizens over 85 increased by more than 100 percent. In 2013 the number of centenarians (those 100 years or older) in Canada was 6,900, almost 20 centenarians per 100,000 persons, compared to 11 centenarians per 100,000 persons in 2001 (Statistics Canada 2013b).
Another reason for the greying of Canada can be attributed to the aging of the baby boomers. Nearly a third of the Canadian population was born in the generation following World War II (between 1946 and 1964) when Canadian families averaged 3.7 children per family (compared to 1.7 today) (Statistics Canada 2012a). Baby boomers began to reach the age of 65 in 2011. Finally, the proportion of old to young can be expected to continue to increase because of the below-replacement fertility rate (i.e., the average number of children per woman). A low birth rate contributes to the higher percentage of older people in the population.
As we noted above, not all Canadians age equally. Most glaring is the difference between men and women; as Figure 13.6 shows, women have longer life expectancies than men. In 2013, there were ninety 65-to-79-year-old men per one hundred 65-to-79-year-old women. However, there were only sixty 80+ year-old men per one hundred 80+ year-old women. Nevertheless, as the graph shows, the sex ratio actually increased over time, indicating that men are closing the gap between their life spans and those of women (Statistics Canada 2013c).

Baby Boomers
Of particular interest to gerontologists right now are the consequences of the aging population of baby boomers, the cohort born between 1946 and 1964 and just now reaching age 65. Coming of age in the 1960s and early 1970s, the baby boom generation was the first group of children and teenagers with their own spending power and therefore their own marketing power (Macunovich 2000). The youth market for commodities such as music, fashion, movies, and automobiles, was a major factor in creating a youth-oriented culture. As this group has aged, it has redefined what it means to be young, middle-aged, and, now, old. People in the boomer generation do not want to grow old the way their grandparents did; the result is a wide range of products designed to ward off the effects—or the signs—of aging. Previous generations of people over 65 were “old.” Baby boomers are in “later life” or “the third age” (Gilleard and Higgs 2007).
The baby boom generation is the cohort driving much of the dramatic increase in the over-65 population. As we can see in Figure 13.7, the biggest bulge in the population pyramid for 2011 (representing the largest population group) is in the age 45 to 55 cohort. As time progresses, the population bulge moves up in age. In 2011 the oldest baby boomers were just reaching the age at which Statistics Canada considers them elderly. In 2020, we can predict, the baby boom bulge will continue to rise up the pyramid, making the largest Canadian population group between 65 and 85 years old.

This aging of the baby boom cohort has serious implications for society. Health care is one of the areas most impacted by this trend. For years, hand-wringing has abounded about the additional burden the boomer cohort will place on the publicly funded health care system. The report by the Commission on the Future of Health Care in Canada noted in 2001 that the combined public and private expenditure per person each year for medical care was approximately three times as much for persons over 65 than for the average person ($10,834 per person versus $3,174). As health care costs increase with age, the reasoning is that more people entering the 65 and older age group will increase the cost of medical care dramatically. In fact, the cost to the health care system specifically due to aging is projected to be no more than 1 percent per year (Romanow 2002). The main sources of cost increase to the health care system come from inflation, rising overall population, and advances in medical technologies (new pharmaceutical drugs, surgical techniques, diagnostic and imaging techniques, and end-of-life care). With respect to end-of-life care, the average Canadian now receives approximately one and a half times more health care services than the average Canadian did in 1975 (Lee 2007). Even with modest economic growth, existing levels of health care service can be maintained without difficulty if the total increase in costs of health care from all sources, including aging, result in an annual increase in health care budget expenditures of 4.4 percent over the medium term as expected (Lee 2007). (Is that why they started paying for sex changes in prisoners, and children, abortions, as well as for all medical expenses for all the immigrants they are bringing into our country?)
Other studies indicate that aging boomers will bring economic growth to the health care industries, particularly in areas like pharmaceutical manufacturing and home health care services (Bierman 2011). Further, some argue that many of our medical advances of the past few decades are a result of boomers’ health requirements. Unlike the elderly of previous generations, boomers do not expect that turning 65 means their active lives are over. They are not willing to abandon work or leisure activities, but they may need more medical support to keep living vigorous lives. This desire of a large group of over-65-year-olds wanting to continue with a high activity level is driving innovation in the medical industry (Shaw 2012). It is not until the final year of life that health care expenditures undergo a dramatic increase. Approximately one-third to one-half of a typical person’s total health care expenditures occur in the final year of life (Lee 2007). The implication is that with people living increasingly longer and healthier lives, the issue of the cost of health care and aging needs to be refocused on end-of-life care options.
The economic impact of aging boomers is also an area of concern for many observers. Although the baby boom generation earned more than previous generations and enjoyed a higher standard of living, they also spent their money lavishly and did not adequately prepare for retirement. (Not quite accurate. Well, at least for Americans. Many baby boomers lost their retirement when their companies were bought out, and in the past few decades there have been no retirement benefits offered and no raises. Many boomers were sold on the idea that they could use a balloon Mortgage because surely they could expect their income to increase, or at least that is what they were told. Then when the balloon payments came due, there was no way for them to meet the increase and they lost their homes. And of course the cost of living just keeps rising and jobs have all but disappeared first going overseas to save the Big Corporation from the expense of paying Americans not to mention the taxes. Then the jobs continued to be lost to foreigners coming to the US on green card lotteries and political bargaining, college paid for and jobs guaranteed. Now even more are being forfeited to all the immigrants who were also promised education, jobs and housing.) According to a 2013 report from the Bank of Montreal, the average baby boomer falls about $400,000 short of adequate savings to maintain their lifestyles in retirement. (Shoot, most people don’t have enough savings to cover emergency expenses like car repairs or hospitalization, let alone $400,000 for retirement) The average senior couple spends approximately $54,000 a year, requiring accumulated savings of $1,352,000 to sustain themselves (not taking into account Canada Pension Plan and Old Age Pension payments). Canadian boomers anticipated they needed savings of $658,000 to feel financially secure in retirement but had only saved an average of $228,000. Seventy-one percent of boomers said they plan to work part time in retirement (BMO Financial Group 2013). This will have a ripple effect on the economy as boomers work and spend less.
Aging around the World

From 1950 to approximately 2010, the global population of individuals age 65 and older increased by a range of 5 to 7 percent (Lee 2009). This percentage is expected to increase and will have a huge impact on the dependency ratio: the number of productive working citizens to non-productive (young, disabled, elderly) (Bartram and Roe 2005). One country that will soon face a serious aging crisis is China, which is on the cusp of an “aging boom”: a period when its elderly population will dramatically increase. The number of people above age 60 in China today is about 178 million, which amounts to 13.3 percent of its total population (Xuequan 2011). By 2050, nearly a third of the Chinese population will be age 60 or older, putting a significant burden on the labour force and impacting China’s economic growth (Bannister, Bloom, and Rosenberg 2010).
As health care improves and life expectancy increases across the world, elder care will be an emerging issue. Wienclaw (2009) suggests that with fewer working-age citizens available to provide home care and long-term assisted care to the elderly, the costs of elder care will increase.
Worldwide, the expectation governing the amount and type of elder care varies from culture to culture. For example, in Asia the responsibility for elder care lies firmly on the family (Yap, Thang, and Traphagan 2005). This is different from the approach in most Western countries, where the elderly are considered independent and are expected to tend to their own care. It is not uncommon for family members to intervene only if the elderly relative requires assistance, often due to poor health. Even then, caring for the elderly is considered voluntary. In North America, decisions to care for an elderly relative are often conditionally based on the promise of future returns, such as inheritance or, in some cases, the amount of support the elderly provided to the caregiver in the past (Hashimoto 1996).
These differences are based on cultural attitudes toward aging. In China, several studies have noted the attitude of filial piety (deference and respect to one’s parents and ancestors in all things) as defining all other virtues (Hamilton 1990; Hsu 1971). Cultural attitudes in Japan prior to approximately 1986 supported the idea that the elderly deserve assistance (Ogawa and Retherford 1993). However, seismic shifts in major social institutions (like family and economy) have created an increased demand for community and government care. For example, the increase in women working outside the home has made it more difficult to provide in-home care to aging parents, leading to an increase in the need for government-supported institutions (Raikhola and Kuroki 2009).
In North America, by contrast, many people view caring for the elderly as a burden. Even when there is a family member able and willing to provide for an elderly family member, 60 percent of family caregivers are employed outside the home and are unable to provide the needed support. At the same time, however, many middle-class families are unable to bear the financial burden of “outsourcing” professional health care, resulting in gaps in care (Bookman and Kimbrel 2011). Chinese Canadians, for example, are thought to have a higher sense of filial responsibility and to perceive providing family assistance for the elderly as a more normal aspect of life than Caucasian Canadians (Funk, Chappell, and Liu 2013). It is important to note that even within a country, not all demographic groups treat aging the same way. While most Americans are reluctant to place their elderly members into out-of-home assisted care, demographically speaking, the groups least likely to do so are Latinos, African Americans, and Asians (Bookman and Kimbrel 2011).
Globally, Canada and other wealthy nations are fairly well equipped to handle the demands of an exponentially increasing elderly population. However, peripheral and semi-peripheral nations face similar increases without comparable resources. Poverty among elders is a concern, especially among elderly women. The feminization of the aging poor, evident in peripheral nations, is directly due to the number of elderly women in those countries who are single, illiterate, and not a part of the labour force (Mujahid 2006).
In 2002, the Second World Assembly on Aging was held in Madrid, Spain, resulting in the Madrid Plan, an internationally coordinated effort to create comprehensive social policies to address the needs of the worldwide aging population. The plan identifies three themes to guide international policy on aging: 1) publically acknowledging the global challenges caused by, and the global opportunities created by, a rising global population; 2) empowering the elderly; and 3) linking international policies on aging to international policies on development (Zelenev 2008).
The Madrid Plan has not yet been successful in achieving all its aims. However, it has increased awareness of the various issues associated with a global aging population, as well as raising the international consciousness to the way that the factors influencing the vulnerability of the elderly (social exclusion, prejudice and discrimination, and a lack of socio-legal protection) overlap with other developmental issues (basic human rights, empowerment, and participation), leading to an increase in legal protections (Zelenev 2008).
13.2. The Process of Aging
What may be surprising is how few studies were conducted on death and dying prior to the 1960s. Death and dying were fields that had received little attention until psychologist Elisabeth Kübler-Ross began observing people who were in the process of dying. As Kübler-Ross witnessed people’s transition toward death, she found some common threads in their experiences. She observed that the process had five distinct stages: denial, anger, bargaining, depression, and acceptance. She published her findings in a 1969 book called On Death and Dying. The book remains a classic on the topic today.
Kübler-Ross found that a person’s first reaction to the prospect of dying is denial, characterized by not wanting to believe that he or she is dying, with common thoughts such as “I feel fine” or “This is not really happening to me.” The second stage is anger, when loss of life is seen as unfair and unjust. A person then resorts to the third stage, bargaining: trying to negotiate with a higher power to postpone the inevitable by reforming or changing the way he or she lives. The fourth stage, psychological depression, allows for resignation as the situation begins to seem hopeless. In the final stage, a person adjusts to the idea of death and reaches acceptance. At this point, the person can face death honestly, regarding it as a natural and inevitable part of life, and can make the most of their remaining time.
The work of Kübler-Ross was eye-opening when it was introduced. It broke new ground and opened the doors for sociologists, social workers, health practitioners, and therapists to study death and help those who were facing death. Kübler-Ross’s work is generally considered a major contribution to thanatology: the systematic study of death and dying.
Of special interests to thanatologists is the concept of “dying with dignity.” Modern medicine includes advanced medical technology that may prolong life without a parallel improvement to the quality of life one may have. In some cases, people may not want to continue living when they are in constant pain and no longer enjoying life. Should patients have the right to choose to die with dignity? Dr. Jack Kevorkian was a staunch advocate for physician-assisted suicide: the voluntary or physician-assisted use of lethal medication provided by a medical doctor to end one’s life. Physician-assisted suicide is slightly different from euthanasia, which refers to the act of taking someone’s life to alleviate that person’s suffering, but that does not necessarily reflect the person’s expressed desire to commit suicide.
This right to have a doctor help a patient die with dignity is controversial. In the United States, Oregon was the first state to pass a law allowing physician-assisted suicides. In 1997, Oregon instituted the Death with Dignity Act, which required the presence of two physicians for a legal assisted suicide. This law was successfully challenged by U.S. Attorney General John Ashcroft in 2001, but the appeals process ultimately upheld the Oregon law. Subsequently, both Montana and Washington have passed similar laws.
In Canada, physician-assisted suicide is illegal, although suicide itself has not been illegal since 1972. On moral and legal grounds, advocates of physician-assisted suicide argue that the law unduly deprives individuals of their autonomy and right to freely choose to end their own life with assistance; that existing palliative care can be inadequate to alleviate pain and suffering; that the law discriminates against disabled people who are unable, unlike able-bodied people, to commit suicide by themselves; and that assisted suicide is taking place already in an informal way, but without proper regulations. Those opposed argue that life is a fundamental value and killing is intrinsically wrong, that legal physician-assisted suicide could result in abuses with respect to the most vulnerable members of society, that individuals might seek assisted suicide for financial reasons or because services are inadequate, and that it might reduce the urgency to find means of improving the care of people who are dying (Butler, Tiedemann, Nicol, and Valiquet 2013).
There are two main legal reference points for the issue in Canada. One is the case of Robert Latimer, the Saskatchewan farmer convicted in 1997 for the mercy killing (or euthanasia) of his 12-year-old daughter, Tracey Latimer, who had a severe form of cerebral palsy, and was unable walk, talk, or feed herself. The second case is that of Sue Rodriguez who sought the legal right to have a physician-assisted suicide because she suffered from ALS (amyotrophic lateral sclerosis). She argued in the Supreme Court that the law against physician-assisted suicide violated her right to “life, liberty, and security of the person” but lost her case in a five-to-four decision in 1992. She did choose physician-assisted suicide two years later from an anonymous physician. In 2012, however, a B.C. court found that the law did discriminate against those who are “grievously and irremediably ill” in the case of Gloria Taylor, another woman with ALS. The court granted a constitutional exemption to permit her to seek physician-assisted suicide while the constitutional challenge to the law is clarified. However, Taylor died from an infection in 2012. The constitutional challenge to the law remains unresolved. In Quebec, the Select Committee on Dying with Dignity tabled a report in 2012 that supported assisted suicide. In 2013 a panel of experts appointed by the Quebec government agreed that in certain circumstances assisted suicide should be understood as part of the continuum of care (Butler et al. 2013). In 2014, Quebec became the first province in Canada to pass right-to-die legislation. Terminally ill adults of sound mind may request continuous palliative sedation that will lead to death (Seguin 2014).
The controversy surrounding death with dignity laws is emblematic of the way our society tries to separate itself from death. Health institutions have built facilities to comfortably house those who are terminally ill. This is seen as a compassionate act, helping relieve the surviving family members of the burden of caring for the dying relative. But studies almost universally show that people prefer to die in their own homes (Lloyd, White, and Sutton 2011). Is it our social responsibility to care for elderly relatives up until their death? How do we balance the responsibility for caring for an elderly relative with our other responsibilities and obligations? As our society grows older, and as new medical technology can prolong life even further, the answers to these questions will develop and change.
The changing concept of hospice is an indicator of our society’s changing view of death. Hospice is a type of health care that treats terminally ill people when cure-oriented treatments are no longer an option (Canadian Hospice Palliative Care Association N.d.). Hospice doctors, nurses, and therapists receive special training in the care of the dying. The focus is not on getting better or curing the illness, but on passing out of this life in comfort and peace. Hospice centres exist as places where people can go to die in comfort, and increasingly, hospice services encourage at-home care so that someone has the comfort of dying in a familiar environment, surrounded by family (Canadian Hospice Palliative Care Association N.d.). While many of us would probably prefer to avoid thinking of the end of our lives, it may be possible to take comfort in the idea that when we do approach death in a hospice setting, it is in a familiar, relatively controlled place.
spacer
Some of the reasons and the forces behind the make up of our current population.
Check out the following related posts:
The BEGINNING OF THE END – Part 1; Part 2, Part 3, Part 3a; Part 4; Part 5; Part 6; Part 7; Part 8
spacer
World War II

spacer
spacer
![]()
3.94M subscribers
spacer
Check out the following related post:
DWAVE – ADAPTING EARTH FOR THE ARRIVAL OF THE FALLEN
spacer
![]()
657K subscribers
Links: – The Asianometry Newsletter: https://www.asianometry.com – Patreon:  / asianometry – Threads: https://www.threads.net/@asianometry – Twitter:
/ asianometry – Threads: https://www.threads.net/@asianometry – Twitter:  / asianometry
/ asianometry
spacer
If you would like to know more about how far back the work on Artificial Intelligence goes click the link below:
Having watched the video above, you might come away thinking that AI was first invented in 1955. Not so, only the TERM: ARTIVICIAL INTELLIGENCE was coined at that time. As you will see below, machines capable of thinking and problem solving were already in existence long before 1955.
spacer
 |
|
Related Article


Yes it did in 1981 !!! I saw pictures of it, and I got the pictures through a man named Ron Carlson, he used to work for the CIA ! I could dig up his tapes on it if I had to. they’re in my office somewhere … he gave a lot of details about it … they may have changed the name of it by now ..?actually it was an acrostic that spelled Beast and there are at least three other huge supercomputers on the globe, that are big like it, also !!!

Yes it does or did. I worked for the company that runs it. I retired from there five years ago and worked in IT Communications. Brussels was the main hub of the global central banks. I actually worked on the original brands called B6700 and B6800 configuring them for sales in NYC the largest revenue producer for the global company. The term emanated from the engineers who were burdened with the cable strapping putting that ‘beast’ together. You can probably find information on Burroughs Bxxx systems on Wikipedia. Of course since the 60s, 70s, 80s, technology has come light years. I do know they were running the old ‘Swift’ banking system that transferred funds globally. They were still actually running fax machine authentication when I left. Sounds antique but that was the only way to securely verify. I always drove AT&T crazy when another fax hub went down because with everything going VoIP international faxes were very problematic. Everything is changing in the banking world with CBDC central bank digital currency versus the QFS Quantum Financial System. There’s a big fight right now on who will win out. If CBDC loses then that’s the end of western Rothschilds fiat currency with everything going instead to asset backed with the BRICS, Brazil, Russia, India, China, South Africa and now Saudi Arabia, more than half the global population. Keep an eye on the war in Ukraine and who wins out and Turkey’s incursion into Syria and Libya to take out the banking cartels there.

Yes, there is. I had heard of such a thing through “Christian” pamphlets in the early 1990s but was unable to validate the truth of it. So i travelled to “Brussels” to see for myself. Where i found blocks and blocks of buildings without windows and only openings for ventilation. The same as is found on “ATT” buildings which house servers that access the world wide web. It was enough to satisfy me…
 A Russian Orthodox leaflet: “Prophecies are coming true:
A Russian Orthodox leaflet: “Prophecies are coming true: spacer
European Supercomputer installed at CERN

spacer
Zurich, Switzerland, 12 December 2002—Switzerland’s fastest computer has been installed at IBM’s Research Laboratory in Rüschlikon near Zurich. Ranked 70 among the world’s top 500 computers, the system works at a top speed of more than a trillion operations per second. The computer will be used by IBM scientists to advance research in computational biochemistry and material sciences. Sophisticated algorithms running on the supercomputer are used to model the behavior of matter on the atomic scale.
Modeling is crucial to understand the chemical and physical processes that take place at the interface of different materials in a multicomponent device, for example, or the way pharmaceuticals interact in the human body. It is the basis for efficiently designing new materials and pharmaceutical compounds.
“The new supercomputer is a tremendous asset for IBM scientists and a powerful showcase for IBM’s supercomputing technology,” says Krishna Nathan, director of IBM Research – Zurich. “We have some of the world’s top experts in computer simulations. The new supercomputer will help them advance their research.”
“These calculations require sophisticated software algorithms and massive parallel computing power because of the huge amount of data and number of process steps to be computed for a reliable simulation of any real system,” says Wanda Andreoni, head of the computational biochemistry and materials science effort at IBM Research – Zurich. “Additional computation power will allow us to tackle more complex systems and to monitor their behavior over longer time scales. It will also permit faster screening of molecular structuresstored in databases.”
Zurich scientists are constantly demonstrating the value of their work in research projects both for IBM and industrial partners in the framework of IBM Research’s Deep Computing projects. Examples at Zurich include the design of novel materials for organic electronics, simulating how progesterone (Progesterone is a hormone that supports menstruation and maintaining a pregnancy ) interacts with its receptor in the human body, and identifying the molecules responsible for the degradation of flavor in foods.
Technical details
The new supercomputer system of IBM’s eServer p690 series deploys a total of 260 Power4 processors that work at a clock speed of 1.3 GHz and perform four floating-point operations (flops*) per cycle. This leads to a theoretical peak performance of 5.2 Gflops per processor, or a top system speed of 1.35 Tflops. The system consists of nine linked units with a total memory capacity of 516 GB of random-access memory (RAM). The eight shared-memory processor (SMP) nodes are interconnected by Gigabit Ethernet switches, which allow links between any two nodes at a maximum speed of 1 Gigabit per second. The system also includes 2.19 TB of disk space stored on 30 disks of 73 Gigabyte capacity each. General Parallel File System (GPFS) is the software that allows very fast, parallel reading and writing, and enables the entire disk space to be used as one unit.
Rank 70 among the world’s top 500 machines (list of November 2002) was determined by LINPACK, a widely accepted benchmark among experts for estimating the “real” performance of a supercomputer. The machine will lead to a doubling of Switzerland’s aggregate installed computer power of systems included in the top 500 list. Another system providing similar performance is the IBM supercomputer at the Swiss National Scientific Computing Center in Manno, ranked number 73.
* A floating point operation represents the multiplication of two numbers with 1 place before and 15 places after the decimal point; floating point operations per second (flops) is a standard measure of computing speed.
*mer- | Etymology of root *mer- by etymonline

Thanatology Definition & MeaningMerriam-Webster
https://www.merriam-webster.com › dictionary › thanat…
than·a·tol·o·gy ˌtha-nə-ˈtä-lə-jē
: the description or study of the phenomena of death and of psychological mechanisms for coping with them.
In Greek mythology, Thanatos was the personification of death and the twin brother of Hypnos (Sleep). The ancient Greeks eventually came to use thanatos as a generic word for “death.” Thanatology is a direct linguistic heir of the Greek term and was first documented in English in the mid-1800s (during the industrial revolution and the Elizabethan craze of spiritism). As a science, thanatology examines attitudes toward death, the meaning and behaviors of bereavement and grief, and other matters. In 1935, the word thanatos itself made its debut in English, ushered in with psychoanalytic theory to describe an unconscious tendency toward self-destruction.
|
| Thanatos Greek Gods / Thanatos Thanatos was the daemonic representation of death in Ancient Greek mythology. He did not play a major part in Greek mythology and rarely appeared in any stories, as he was mostly displaced by Hades, the god of the Underworld. He was the son of Nyx (the Night) and Erebus (the Darkness), while his twin brother was Hypnos (the Sleep). Other siblings of Thanatos and Hypnos included Geras (old age), Eris (strife), Nemesis (retribution), Apate (deception) and Charon (the boatman that led the souls to the Underworld). Thanatos was believed to be merciless and indiscriminate, and both mortals and gods hated him. However, he could sometimes be outsmarted. In a myth, Thanatos was told by Zeus to chain King Sisyphus in the Underworld, as it was time for him to die. Sisyphus managed to chain Thanatos in his own fetters, thus protecting all mortals from dying while the god was chained. In the end, god Ares, angry that at the wars he waged noone died, freed Thanatos and gave Sisyphus to him. |
| thanatology (n.) |
euthanasia (n.) |
spacer
Check out the related post:
Cannibal Zombie Apocalypse is FORMING
SPACER
Soylent Green Documentary – A Look at the World of Soylent Green
![]()
9.84K subscribers
Soylent Green is a 1973 American science fiction film directed by Richard Fleischer and starring Charlton Heston and, in his final film, Edward G. Robinson. The film overlays the police procedural and science fiction genres as it depicts the investigation into the murder of a wealthy businessman in a dystopian future suffering from pollution, overpopulation, depleted resources, poverty, dying oceans, and a hot climate due to the greenhouse effect. Much of the population survives on processed food rations, including “soylent green”. The film, which is loosely based upon the 1966 science fiction novel Make Room! Make Room!, by Harry Harrison, won the Nebula Award for Best Dramatic Presentation and the Saturn Award for Best Science Fiction Film in 1973. “Copyright Disclaimer Under Section 107 of the Copyright Act 1976, allowance is made for “fair use” for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. Fair use is a use permitted by copyright statute that might otherwise be infringing. Non-profit, educational or personal use tips the balance in favor of fair use.” www.twitch.tv/altplanes3001
google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwjs46CSifSFAxVaAzQIHUxdABIQwqsBegQIFRAG&url=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3DqyizAHAbPII&usg=AOvVaw3uMDCRJGNMb7fDl2W0dte9&opi=89978449


Ephesians 5:11, 13-16: “And have no fellowship with the unfruitful works of darkness, but rather reprove them. But all things that are reproved are made manifest by the light: for whatsoever doth make manifest is light. Wherefore he saith, Awake thou that sleepest, and arise from the dead, and Christ shall give thee light. See then that ye walk circumspectly, not as fools, but as wise, Redeeming the time, because the days are evil.”
The 1828 Noah Webster Dictionary defines: “Reprove”: To blame, to convince of a fault, or to make it manifest, to excite a sense of guilt.“Circumspectly”: Cautiously; with watchfulness every way; with attention to guard against surprise or danger.
Matthew 24:24: “...if it were possible, they shall deceive the very elect.”
II Corinthians 2:11: “Lest Satan should get an advantage of us: for we are not ignorant of his devices.”
II Chronicles 7:14: “If my people, which are called by my name, shall humble themselves, and pray, and seek my face, and turn from their wicked ways; then will I hear from heaven, and will forgive their sin, and will heal their land.”
Luke 21:36 Watch ye therefore, and pray always, that ye may be accounted worthy to escape all these things that shall come to pass, and to stand before the Son of man.
Matthew 24:13 But he that shall endure unto the end, the same shall be saved.
Psalm 101:3: I will set no wicked thing before mine eyes: I hate the work of them that turn aside; it shall not cleave to me.
Psalm 11:5: The LORD trieth the righteous: but the wicked and him that loveth violence his soul hateth.
1 Cor 15:33: Be not deceived: evil communications corrupt good manners. Lexicon Strong’s G3657–Outline of Biblical Usage of the Word: “Communications”: companionship, communion
“It does not take a majority to prevail… but rather an irate, tireless minority, keen on setting brushfires of freedom in the minds of men.” Samuel Adams “The average age of the world’s great civilizations has been two hundred years. These nations have progressed through the following sequence: from bondage to spiritual faith, from spiritual faith to great courage, from courage to liberty, from liberty to abundance, from abundance to selfishness, from selfishness to complacency from complacency to apathy, from apathy to dependency, from dependency back to bondage.” Alexander Fraser Tytler
spacer
check out the following related post:
WHAT?? CANNIBALISM TO SAVE THE WORLD? ARE WE COMPLETELY INSANE???
spacer
SICK: Climate Scientist Suggests “Culling” the Human Population with a Deadly Pandemic to Solve the “Climate Crisis”

One government climate scientist made the mistake of blurting out the real end-game of so many radical environmental activists in a bid to preserve the planet: Killing off the human population.
Bill McGuire, a Professor of Geophysical & Climate Hazards at University College London (UCL), authored a tweet Sunday that lamented the fact carbon emissions were not falling nearly as fast as needed and suggested solving the “climate crisis” with a deadly pandemic to wipe out swaths of the human population.
“If I am brutally honest, the only realistic way I see emissions falling as fast as they need to, to avoid catastrophic #climate breakdown, is the culling of the human population by a pandemic with a very high fatality rate,” he wrote.
|


After righteous backlash from social media users, McGuire deleted his post and whined that people were deliberately taking his words out of context.


He then lied and claimed that his initial post was about falling economic activity despite clearly referencing a pandemic killing off mankind.
As the National Pulse notes, McGuire is infamous for being a member of a British government body that advised politicians on the COVID-19 response. He also co-authored a report for the radical United Nations’s Intergovernmental Panel on Climate Change (IPCC), which helps influence climate policy worldwide.
McGuire is also not the first leftist to suggest exterminating the human population to solve the planet’s issues. For example, infamous animal rights activist Jane Goodall once floated reducing the Earth’s population to what it was 500 years ago. A University of Texas professor also called for killing 90 PERCENT of all humans to save the planet.
American taxpayers are also funding risky Chinese research on the bird flu more transmissible, a disease that kills over 50% of the people it infects. COVID-19, by comparison, has a fatality rate of less than 1%.
These facts add fuel to the theory that COVID-19 was created as a trial run and globalists are planning to develop a far more deadly virus to provide a “final solution” to the human race.
spacer
Save the Planet, Kill Yourself
Over the past few weeks I’ve been really into researching religious zealots and cults (brought on by this Netflix documentary called Jesus Camp –10/10 would recommend) and I just read an article about one group in particular that shocked me a little more than all the rest. The Church of Euthanasia was founded in the mid-1990s by an ex-DJ named Chris Korda, who says the church’s guiding principle is “Thou shalt not procreate.”Apparently, Korda and her followers (of which there were more than I had hoped) were so worried about climate change and overpopulation that they decided to start a movement based solely on encouraging people to die.

“Fetuses AREN’T People. They aren’t even CHICKENS. Who Cares?”
The Church of Euthanasia gained traction by protesting at major political events, including the 1992 Democratic National Convention, where they popularized their slogan, “Save the Planet, Kill Yourself.” This fits in nicely with the four pillars of their religion, which are as follows: “Suicide (optional but encouraged), abortion (may be required to avoid procreation), cannibalism (mandatory if you insist on eating flesh, but only if someone is already dead), and sodomy (optional, but strongly encouraged).” It seems as though the CoE was trying to get rid of the Earth’s population through every way possible, except outright homicide. Side note: I’m a little unsure of where cannibalism fits into the whole philosophy, but I guess that by consuming dead bodies you’re freeing up space for other activities???
The part that really shocked me was the hotline the Church attempted to set up, which would have provided round the clock instructions for people looking to commit suicide. It’s kind of a cruel twist of fate, because suicide hotlines are normally resources used to prevent suicide, not to encourage it. I really couldn’t believe that people’s lives meant so little to the members of this group that they were willing to encourage this sort of behavior for the sake of an imperceptible amount of extra breathing room on the planet.
I was expecting a disclaimer at the end of the article, something along the lines of, “Korda, along with her most loyal followers, committed suicide in 1995..,” but there was none. The founder of the Church of Euthanasia, who had no problem telling everyone else it was their duty to die, is still living today.Whether that means she felt she needed to be here to keep up the mission, or if the whole thing was just some elaborate hoax, I don’t know.
Link to article: http://www.vice.com/read/save-the-planet-kill-yourself-the-contentious-history-of-the-church-of-euthanasia-1022
This article is part of a Vice News column called “Post Mortem” and there are some really great pieces on there as well!
spacer
spacer
Please check out the following related posts:
PANDEMIC – OUTBREAK – Diseases, Epidemics, Pandemics and Plagues
LET’S HAVE A SERIOUS TALK ABOUT EPIDEMICS!; and
Part 2 – Candida Auris
WHEN DO WE SAY – ENOUGH!!
Welcome to YOUR FUTURE – Medical Tyranny
BILL GATES IN HIS OWN WORDS – EUGENICS BY ANY MEANS
CLOSING COMMENTS:
Once you are broke, penniless and have lost your home you will be at the mercy of the Government. They will provide what you need to live as long as you follow their commands, most especially when it comes to your health. You will eat what they tell you, drink what they allow, you will see the doctor that is assigned to you, take the medications recommended for you, follow the immunization schedules, exercise, and sleeps when and how you are told. They way they will know if you are doing as you are told is by the feedback they get from the nanobots in your system. You will do as your told or lose your healthcare. If you lose your healthcare you will be ostracized from the community. You will not be allowed housing, food, clothing or medications. In other words you will be left to die.
spacer